last updated:
April 1, 2026
min read
Understanding PCOS-related fertility challenges




PCOS and fertility can feel confusing, but the truth is that many people with PCOS do get pregnant. Understanding how PCOS affects ovulation, hormones, and treatment options can help you figure out where you are in the process and what steps might help next.
When you’re thinking about getting pregnant, PCOS and fertility can feel like a confusing, emotional maze. Maybe your cycles are unpredictable, maybe you’ve heard that polycystic ovarian syndrome (PCOS) causes infertility, or maybe you’ve already spent months trying without success. It’s a lot to carry, and it’s completely normal to feel anxious, frustrated, or discouraged.
Here’s the good news: while PCOS is one of the leading causes of infertility, it does not mean you can’t get pregnant. In fact, many people with PCOS go on to conceive—sometimes naturally, sometimes with a little medical support along the way.
While I don’t personally have PCOS, I do know what it’s like to struggle with getting pregnant. I became a mom in my forties, and I remember how overwhelming it felt to sort through conflicting advice and unclear information. When you’re making decisions about fertility, clear, medically accurate guidance matters because it helps you understand your body and choose your next steps with more confidence.
So, if you’ve been Googling terms like PCOS and infertility or wondering about your chances of getting pregnant with PCOS, you’re in the right place. In this guide, we’ll walk through how PCOS actually affects fertility, what the research says about real-world pregnancy odds, PCOS infertility rates, and the step-by-step treatment pathway doctors often use to help people conceive. We’ll also cover when it makes sense to seek help from a fertility specialist and how to know when it’s time to move beyond trying on your own.
If you’re navigating PCOS and hoping to grow your family, you’re not alone and understanding what’s happening in your body is the first step toward figuring out what comes next.
PCOS is one of the most common causes of infertility. In fact, it accounts for about 18% of infertility cases overall and up to 80% of infertility linked to ovulation problems.
But this isn’t meant to scare you—it’s meant to give you clarity. Knowing how PCOS can affect fertility helps you and your provider pinpoint what’s going on and choose the right strategy to improve your chances of pregnancy.
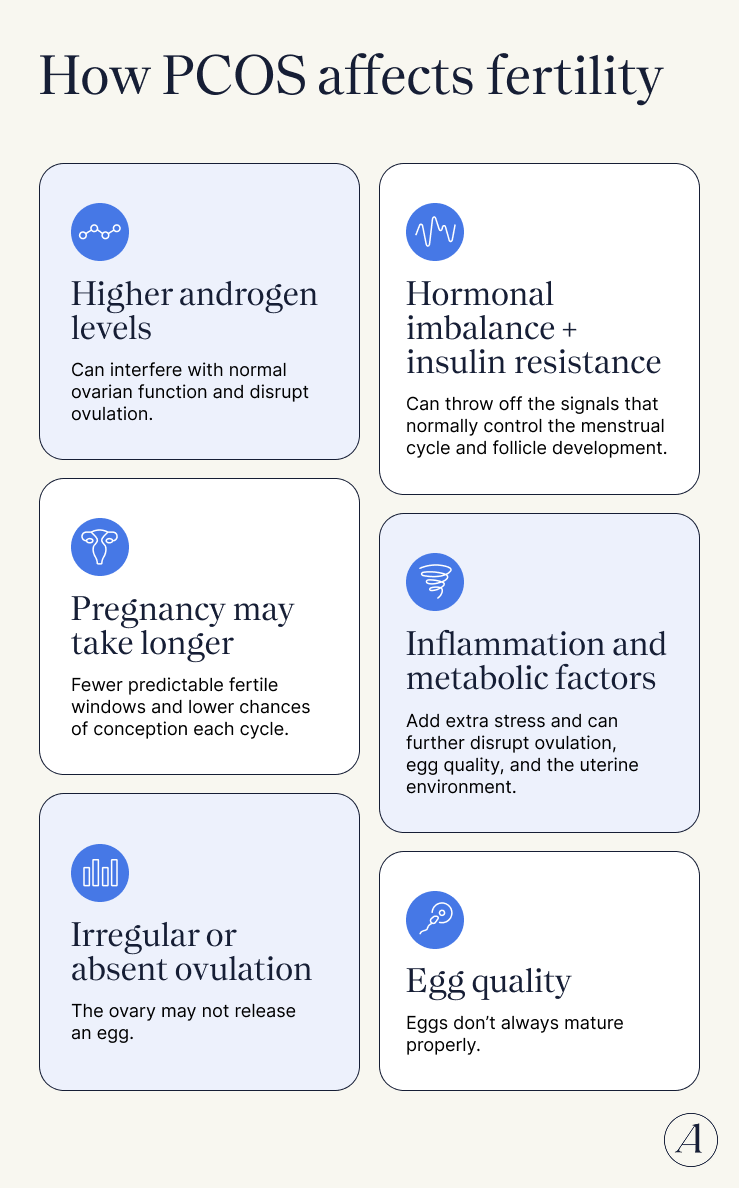
So, what exactly is happening in the body? Let’s break down the main ways PCOS can make conception harder and what those challenges actually look like.
Failure to ovulate is the most common cause of female infertility overall. About 40% of women with infertility issues experience ovulation problems, and among those seeking treatment for anovulation, roughly 90–95% have PCOS. Since pregnancy requires an egg and sperm to meet, ovulation is essential.
In people with PCOS, hormonal imbalances can impact the normal process of growing and releasing an egg from the ovary. Common hormonal shifts that interfere with the ovulatory cycle include:
Together, these shifts can make ovulation unpredictable or absent.
Many people with PCOS have insulin resistance, meaning their cells don’t respond efficiently to insulin—the hormone that helps move glucose from the bloodstream into cells for energy. As a result, the pancreas produces more insulin to keep blood sugar stable. Estimates suggest 35–80% of people with PCOS experience some degree of insulin resistance.
Insulin resistance can directly affect reproduction and has been linked to fertility challenges. In PCOS, “the excess insulin circulating acts synergistically with LH to stimulate the theca cells, which leads to androgen production and irregular ovulation,” says Dr. Huddleston.
In addition to irregular or absent ovulation, insulin resistance can also disrupt reproductive function by leading to:
These metabolic changes may also increase the risk of thrombosis, which can impact embryo development and raise the chances of fertilization failure or miscarriage.
Insulin resistance can influence fertility treatment outcomes as well. It has been associated with lower success rates in assisted reproductive technologies, along with higher risks of spontaneous abortion, gestational diabetes, and other pregnancy complications.
Ovulation alone doesn’t guarantee fertility—egg quality matters, too. Even when someone with PCOS ovulates, fertility challenges can still occur. One reason may be issues with egg (oocyte) quality. In PCOS, eggs don’t always mature the way they should. An immature egg might be released at the wrong time, struggle to travel through the fallopian tube, or fail to fertilize once it meets sperm.
It’s also important not to confuse egg quality with egg quantity. Low egg count—known as diminished ovarian reserve—means the ovaries contain fewer eggs than expected for someone’s age. But PCOS is often the opposite situation. Many people with PCOS actually have a higher-than-average number of eggs in their ovaries. Because ovulation is frequently skipped, those eggs accumulate over time, creating a large ovarian reserve.
Research shows that markers of ovarian reserve—like anti-Müllerian hormone (AMH) levels and antral follicle count (AFC)—tend to be higher in women with PCOS than in similarly aged women who ovulate regularly. These levels also decline more slowly with age in PCOS.
But, unfortunately, a strong egg reserve doesn’t guarantee easy conception. Even with plenty of eggs, other factors linked to PCOS—especially insulin resistance and hormonal imbalance—can still interfere with ovulation, egg development, and overall fertility.
A growing body of research suggests that chronic, low-grade inflammation plays a key role in both the development of PCOS and the fertility challenges that often come with it.
In PCOS, inflammation is closely tied to insulin resistance and metabolic dysfunction. Hormonal disturbances in fat tissue can help trigger insulin resistance, while abnormal glucose and lipid metabolism may cause low-grade inflammation in blood vessels of the reproductive system. In turn, insulin resistance can fuel inflammatory immune responses that interfere with normal ovarian function and stimulate the ovaries to produce excess androgens.
Obesity—also commonly associated with PCOS—can amplify the problem by increasing oxidative stress and inflammatory molecules in the body. Together, these processes may disrupt ovulation and make conception more difficult.
Yes, some people with PCOS can conceive without fertility treatment. The biggest factor is whether you’re ovulating regularly, says Dr. Huddleston. While there’s no official data, she hypothesizes the chances of conceiving may be closer to those of people without PCOS if ovulation is happening consistently.
Because PCOS varies widely, there’s no single fertility statistic, but some estimates suggest that with frequent unprotected sex over a year, about 85% of couples in the general population conceive, compared with around 50% among people with PCOS.
For people who don’t ovulate regularly, natural conception rates are likely to be lower, says Dr. Huddleston. But that doesn’t mean pregnancy can’t happen. If ovulation occurs—even occasionally—there’s still a chance of conceiving. In fact, some people with PCOS assume they can’t get pregnant because their periods are irregular, skip birth control, and end up surprised by an unexpected pregnancy.
Age adds another twist to the PCOS fertility story. Interestingly, many people with PCOS begin having more regular cycles as they get older, particularly in their mid-to-late 30s, according to Dr. Huddleston. But there’s a catch: while people with PCOS often have a larger ovarian reserve, egg quality still declines with age, especially after 35, she adds.
The bottom line: the outlook is often very positive. “The vast majority of patients with PCOS will be able to get pregnant and have a child,” says Dr. Huddleston. Some will conceive naturally, while others may need a little extra support, but in most cases, pregnancy is still very much within reach.
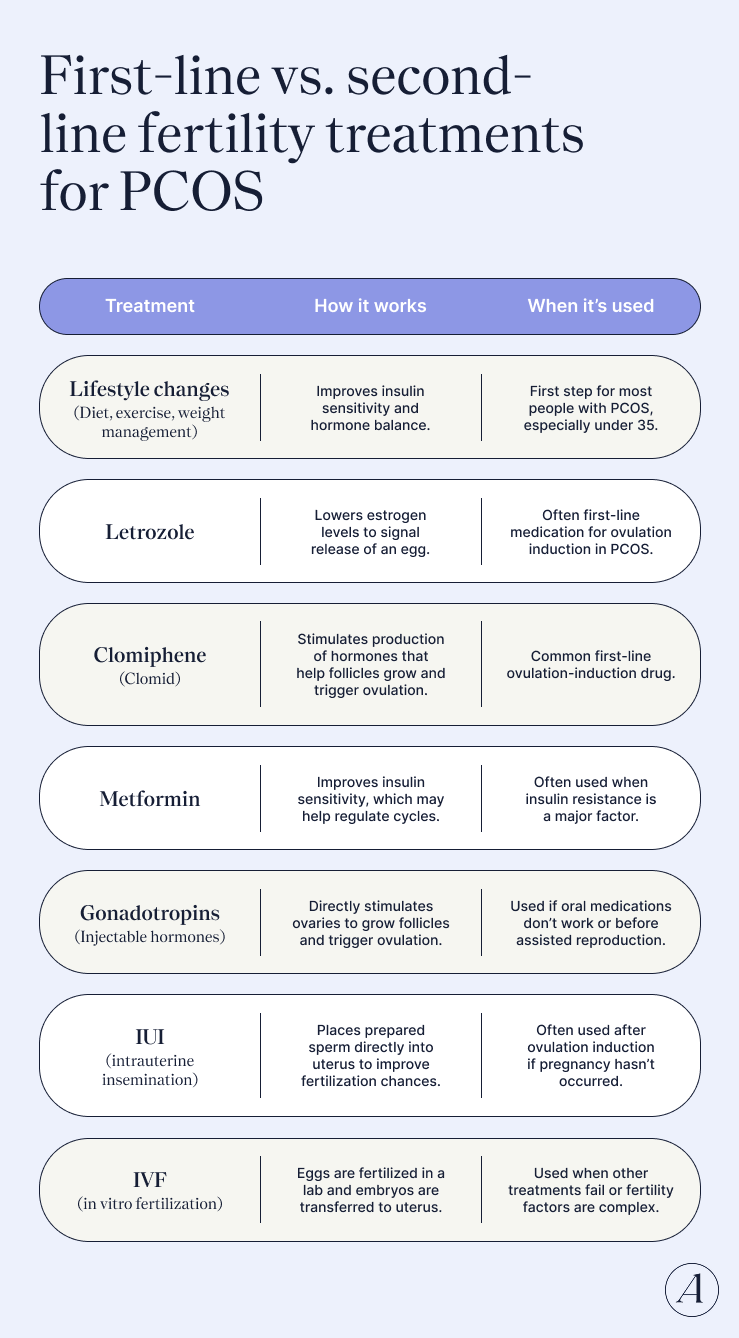
The encouraging part: there’s a lot you can do to support fertility with PCOS. For many people with PCOS—especially those under 35—the first line of treatment focuses on lifestyle changes that support ovulation and metabolic health.
Small, consistent tweaks to your daily routine can help regulate hormones, improve ovulation, and boost your chances of conceiving.
One quick note: If you have PCOS and want to get pregnant, it’s always smart to check in with your healthcare provider early. They can help tailor a plan to your body and pivot to other treatments if lifestyle changes alone aren’t enough.
Exercise helps your muscles absorb glucose, which can reduce high insulin levels (hyperinsulinemia)—a major driver of PCOS symptoms.
Here’s what research suggests:
Weight and PCOS have a complicated relationship, but it can matter for fertility. Not everyone with PCOS has excess weight. But when it is present—especially abdominal fat (central obesity)—it’s linked to higher insulin levels and insulin resistance, which can worsen hormonal and metabolic disruptions.
That cascade can lead to:
For people with overweight or obesity, even a modest 5–10% weight reduction may significantly improve metabolic health and ovulation.
Food choices can help calm the underlying inflammation linked to PCOS and fertility challenges. Many clinicians recommend eating patterns that help reduce inflammation and stabilize blood sugar.
Some studies also suggest that low-glycemic or lower-carbohydrate diets may help improve insulin resistance, menstrual regularity, and fertility outcomes in PCOS.
Foods to limit:
Some studies show improvements in ovulation rates and menstrual cycle regularity in people with PCOS who supplement with inositols.
They work by helping to improve insulin sensitivity and ovarian function. Specifically by:
Though inositol may be a useful adjunct, always talk with your healthcare provider before starting a new supplement.
People with PCOS are more likely to experience sleep challenges, including obstructive sleep apnea, reduced REM sleep, poorer sleep quality, and daytime fatigue.
Poor sleep doesn’t just affect energy—it’s also linked to:
All issues that impact fertility.
Melatonin—the hormone that regulates circadian rhythms and is critical for sleep—may be one piece of the puzzle. Secretion of melatonin appears to be altered in people with PCOS.
Melatonin may:
For this reason, melatonin supplementation may help support both sleep and reproductive function. Ask your provider whether melatonin supplementation might make sense for you.
Low vitamin D levels may worsen PCOS symptoms. Maintaining adequate levels (generally ≥30 ng/mL) may help:
Your provider can test your levels and recommend supplementation if needed.
Your environment can influence hormones more than you might think. Researchers are increasingly studying endocrine-disrupting chemicals (EDCs)—substances that can mimic or interfere with natural hormones—and how they may contribute to PCOS.
EDCs are found in many everyday products, including:
Some evidence suggests these chemicals may disrupt reproductive hormones and increase the risk of PCOS-related fertility challenges. For example, exposure to certain pollutants like polychlorinated biphenyls (PCBs) has been linked to menstrual abnormalities and implantation failure in IVF.
Not everyone exposed to these chemicals develops PCOS or fertility issues, but reducing exposure where possible may be a helpful precaution, especially when trying to conceive.
A step-by-step fertility roadmap for PCOS
Trying to get pregnant with PCOS can feel overwhelming, but it helps to think of the process as a roadmap—with clear steps that move from understanding your cycle to addressing underlying health issues and exploring fertility treatments for PCOS that can support ovulation and conception.
Ovulation—when the ovary releases an egg—is the key event that makes conception possible. That’s why the first step in any PCOS fertility plan is figuring out whether ovulation is actually happening. There are several simple ways to track it, and many people use a combination for a clearer picture.
Track your cycle
Ovulation typically happens about midway through the menstrual cycle, though timing can vary widely from person to person. Cycle-tracking apps such as (Mira Fertility, Inito, Oova, or Flo) or online ovulation calculators estimate your fertile window based on the first day of your period and your average cycle length.
Just keep in mind: these tools are estimates, not guarantees. And for people with PCOS, irregular cycles can make predictions less reliable. Still, they can be a helpful starting point, “especially if cycles are <35 days,” says Dr. Huddleston. “If cycles are >35 days, there is an increased likelihood that ovulation isn't happening regularly,” she adds.
Pay attention to your body’s clues
Your body often drops hints when ovulation is approaching. Common signs include:
Tracking these signals over time can help you spot patterns in your cycle.
Try an ovulation predictor kit
Over-the-counter ovulation tests detect luteinizing hormone (LH) in your urine. When LH surges, ovulation usually happens within 36 hours.
They’re easy to use—just pee on a test strip at home—and can give you a clearer signal that you’re ovulating.
Track your basal body temperature
Another method is monitoring basal body temperature. During ovulation, body temperature typically rises about 0.5–1°F.
To track it accurately, take your temperature every morning before getting out of bed or eating/drinking, using a thermometer designed for basal body temperature. Recording temperatures over several cycles can help you see when (or if) ovulation tends to occur.
The next step in improving fertility with PCOS is tackling the underlying factors that can throw reproduction off track. PCOS isn’t just an ovarian condition—it’s also a metabolic and hormonal disorder, and those imbalances can make ovulation and conception harder.
Some common PCOS-related issues can interfere with fertility including:
Managing these factors—often through lifestyle changes, medications, or both—can make a big difference. For some people with PCOS, optimizing metabolic health can even “help restore ovulation,” which is critical for creating a more favorable environment for pregnancy, says Dr. Huddleston.
If lifestyle changes aren’t enough to restore ovulation, doctors often turn to fertility medicines for PCOS designed to stimulate the ovaries and regulate hormones. For many people with PCOS, these drugs are the first medical step toward improving fertility.
The bright spot: fertility treatments tend to work especially well when infertility is caused by ovulation problems, like in many cases of PCOS.
Clomiphene
Clomiphene (often called Clomid) is an oral medication that encourages the body to produce more of the hormones that stimulate egg development in the ovaries.
It’s widely used and fairly effective:
One thing to know: clomiphene slightly increases the chance of multiple pregnancy, with about a 10% chance of twins.
Letrozole
Letrozole is another oral medication that works by lowering estrogen levels, which signals the brain to stimulate the ovaries to release eggs. Originally developed for breast cancer, it’s now widely used off-label to support fertility.
Some studies suggest letrozole may actually work better than clomiphene for people with PCOS. In other research on people with unexplained infertility, about 19% of couples achieved a live birth after four months of treatment with letrozole.
Metformin
Metformin is best known as a medication for type 2 diabetes, but it can also play an important role in PCOS treatment.
By improving insulin sensitivity, metformin may:
Some studies even suggest metformin may improve live birth rates in people with PCOS compared with placebo.
If first-line treatments don’t work, there are still effective next steps.
Gonadotropins
Gonadotropins are injectable hormones—such as follicle-stimulating hormone (FSH)—that directly stimulate the ovaries to grow and mature follicles, triggering ovulation.
They’re often used when someone doesn’t respond to oral medications like clomiphene or letrozole, or when preparing for assisted reproductive technologies.
Because they strongly stimulate the ovaries, gonadotropins come with a higher risk of multiple pregnancy:
Intrauterine insemination (IUI)
IUI is a minimally invasive fertility treatment that places prepared sperm directly into the uterus using a thin catheter around the time of ovulation. It’s often combined with ovulation-stimulating medications to improve the chances of pregnancy.
Research suggests IUI can be an effective option for some people with PCOS. In one study:
Compared with IVF, IUI is generally less invasive, less expensive, and less physically demanding, making it a common next step if ovulation induction treatments alone don’t work.
When other options fall short, in vitro fertilization (IVF) may offer another path forward. During IVF, eggs are retrieved from the ovaries and fertilized with sperm in a laboratory. The resulting embryo is then transferred into the uterus, where it may implant and develop into a pregnancy.
Research suggests people with PCOS can respond well to IVF. In one study, women with PCOS aged 35 and older had higher cumulative live birth rates over two years compared with women of similar age and BMI without PCOS. The advantage may stem from having more eggs and embryos available, which can offset some age-related declines in egg quality.
Another study found no significant difference in embryo arrest rates between people with PCOS and those without it. (Embryo arrest refers to embryos that stop developing during an IVF cycle, often due to genetic or metabolic factors.)
That said, IVF success isn’t one-size-fits-all, and outcomes may still depend on key factors like age and body mass index (BMI). Some research shows age remains one of the strongest predictors of success. In one study, IVF success rates were about 43% for people under 35 with PCOS, compared with roughly 16% for those over 35.
Body weight can also play a role. The same research found clinical pregnancy rates in people with obesity were less than half those seen in patients with normal or moderately elevated BMI.
There are also risks to consider, especially for people with PCOS. One potential complication is ovarian hyperstimulation syndrome (OHSS), which occurs when the ovaries overreact to fertility medications and become swollen and painful. Most cases are mild, but severe OHSS—though rare—can lead to serious complications such as blood clots or ovarian torsion.
People with PCOS are more prone to OHSS, but fertility specialists now have strategies to lower the risk. Careful stimulation protocols, along with measures like metformin use and vitamin D optimization before treatment can help make IVF safer and more manageable.
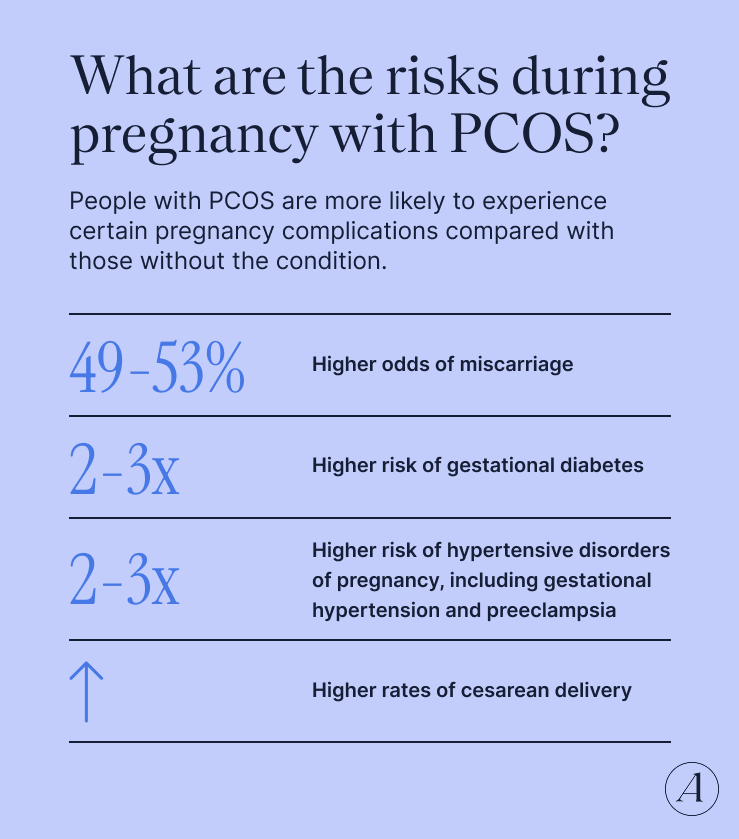
Research shows that people with PCOS are more likely to experience certain pregnancy complications compared with those without the condition.
For example, one study found that people with PCOS have:
There can also be some risks for the baby. Babies born to parents with PCOS are more likely to be larger than average (macrosomia) and may be more likely to spend time in the neonatal intensive care unit (NICU).
Before this sends you into a spiral, take a breath. These statistics highlight potential risks—not guarantees. With good prenatal care, early screening, and close monitoring, many people with PCOS go on to have healthy pregnancies and healthy babies. And knowing these risks ahead of time simply helps you and your provider stay one step ahead.
Trying to conceive with PCOS can feel overwhelming, but it’s important to remember that PCOS doesn’t mean pregnancy is off the table. As Dr. Huddleston explains, “Generally speaking, PCOS is not a reason someone won’t be able to get pregnant.” What it can do, however, is create challenges—often related to ovulation and hormones—that sometimes require a little extra support, she adds.
The hopeful part? Through timely diagnosis, self-education, lifestyle tweaks, and high-quality multidisciplinary care, it’s absolutely possible to take control of PCOS and improve your odds of pregnancy.
If you want to conceive and are wondering where to start, the team at Allara can help. Their multidisciplinary experts investigate symptoms through targeted hormone testing, provide a clear diagnosis, and build a personalized treatment plan designed to help you feel more in sync with your body and optimize your chances of getting pregnant.
Absolutely. The biggest factor is whether you’re ovulating. PCOS often disrupts ovulation, which can make it harder to get pregnant, but it doesn’t mean pregnancy isn’t possible. The key is identifying what’s getting in the way—like hormonal imbalances or insulin resistance—and addressing it.
The peak PCOS fertility rate (with age as a factor) generally follows the same overall pattern as the general population, with the highest PCOS fertility rate in the 20s and early 30s. Interestingly, some people with PCOS may start having more regular cycles in their mid-to-late 30s, which can sometimes improve ovulation. But age still matters—egg quality declines over time, particularly after 35, even if someone with PCOS has a larger ovarian reserve.
Both drugs work by stimulating ovulation, but some research shows letrozole may lead to higher PCOS pregnancy success rates and live-birth rates compared with clomiphene. That said, both medications can be effective, and the best choice depends on your specific situation and your provider’s recommendation.
“I was given an explanation of how my hormonal imbalance was affecting me as a whole - body & mind - & tools so that we could start to manage my condition. I am happy to announce after a year of trying, I found out that I was pregnant & I couldn’t be happier!”


“This is genuinely the first time in my 7 years of being diagnosed, that I have felt seen and heard.”

“The Allara Community gives me the courage and support to continue my PCOS journey - I am never afraid to ask the hard questions and love hearing from other women with the same challenges.”

"My doctor went above and beyond making sure I had all the necessary tests, but also tremendously helped me in understanding my diagnosis, helping me change my lifestyle, and making sure I get the treatment I deserve."

"Before Allara I had no real direction or understanding of what it meant to have PCOS. Now I have a team of people that take time to explain every single thing to me, ask me how I feel and let me be a part of my treatment plan."
